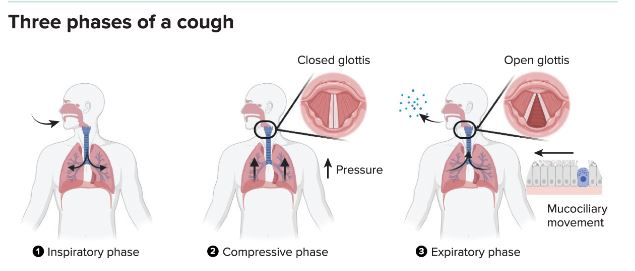
A cough, whether initiated reflexively by sensory neurons in the airway or volitionally, requires three steps. It begins with a quick inhale. That’s immediately followed by closing the glottis at the back of the throat, which allows pressure to build in the lungs. Finally, the glottis opens and releases a high-speed burst of air, along with any particles caught up in the action.
By Alice Callahan, Knowable Magazine
Michael Shiloh had been studying tuberculosis for about two decades when he started wondering about a seemingly basic question: What makes people with TB cough? This is the disease’s hallmark symptom and a main mode of transmission, but despite training as an infectious disease physician and many years of probing the pathogen as a researcher, Shiloh realized that he didn’t know. A quick search of the literature suggested that “essentially nothing had been studied about it, at least not at the molecular level,” he says.
Elucidating the role of cough in illness means first appreciating its role in health. “Cough is one of these critical defensive processes that we have to clear the respiratory system,” says Stuart Mazzone, a neuroscientist at the University of Melbourne. But it also contributes to disease spread, as research by Shiloh, now at the University of Texas Southwestern Medical Center, and others has described. And dysfunctional control of coughing – resulting in too much coughing or not enough – can cause serious health problems.
Here’s a look at how and why we cough, and some of the ways that coughing can go wrong.
What is the cough reflex, and how does it work?
On a recent morning, researcher Karen Hegland literally inhaled part of her breakfast. “I aspirated my coffee, coughed like crazy, but was able to clear my lungs,” says Hegland, a speech-language pathologist who studies coughing and swallowing function at the University of Florida. A common experience, such coughing is a potent reminder of the importance of the reflex Hegland studies. Without her thinking about it, that reflex sprang into action, potentially preventing airway inflammation and infection that can result from breathing in food or drink.
The cough reflex can also be triggered by a range of chemicals, like those contained in cigarette or wildfire smoke, as well as toxic gases and the stomach juice that can sometimes backtrack into the respiratory tract during an episode of acid reflux. When you cough, “your airway, because it’s so important to you, is protecting itself against the damage associated with aspiration of oral gastric contents or noxious materials,” says Shiloh.
Receptors on one of several types of neurons that snake through the lining of the respiratory tract trigger the cough reflex. Some neurons detect chemical stimuli and others are mechanosensory, detecting pressure from something like a bit of food, another foreign object or a liquid like Hegland’s coffee.
When activated, the neurons send signals to the base of the brain – the brainstem – to initiate a cough, which briefly rejiggers normal breathing activity into three quick, coordinated phases. First, a sharp inhale. Then, closing of the space between the vocal cords, called the glottis, and contraction of abdominal and ribcage muscles to build pressure in the chest. Finally, opening of the glottis to release a sudden burst of compressed air.
In addition to this reflexive activity between neurons in the airway and the brainstem, higher-order brain processes add more complexity to the control of coughing; they allow us to cough on purpose, for example, or to sense an urge to cough and at least temporarily suppress it, avoiding an untimely outburst during a key moment in a movie theatre.
Does coughing when you’re sick serve a purpose?
During a respiratory infection, coughing helps to clear accumulating mucus and other secretions, which can prolong infection and, if long-lasting, increase the odds of airway damage. “Cough is a protective thing in those circumstances,” says Anne Chang, a pediatric pulmonologist at Queensland University of Technology in Brisbane, Australia.
But beyond the physical removal of respiratory secretions, it’s still unclear whether coughing helps us fight an infection, and thus whether cough-suppressant medications might slow recovery. It hasn’t been well studied, Shiloh says. Certainly, suppressing the cough might block transmission to other people in your midst and also help you sleep, he says. But, he adds, “maybe you’re keeping the infectious material and inflammatory material in your lung and it’s creating a breeding ground for more organisms. No one knows.”
Whether it’s a good idea to take cough suppressant medications likely depends on whether you have a wet or dry cough. “Blocking a highly productive cough is probably not a wise thing,” says Mazzone. But “a dry, hacking cough is not really serving the purpose of clearance.” Suppressing this type of cough does not seem to be harmful, he says. (Because of the risk of serious side effects, over-the-counter cough suppressants and other cold medicines are not recommended for children under 4, though.)
How do pathogens trigger a cough?
When Shiloh started pondering the root cause of the cough that accompanies a TB infection, he had an inkling that the bacterium that causes it, Mycobacterium tuberculosis, might make molecules that trigger cough sensory neurons. Together with a determined research assistant and other collaborators, he set to work searching for candidates.
After a few dead ends, they identified a molecule called sulfolipid-1, found in the outer membrane and cell wall of the bacterium. When they exposed healthy guinea pigs to aerosolized sulfolipid-1, the animals coughed. But when they were infected with a strain of M. tuberculosis lacking sulfolipid-1, the guinea pigs hardly coughed at all, the team reported in the journal Cell in 2020.
Making sulfolipid-1 may be a strategy on the part of M. tuberculosis to enhance its own transmission to new hosts by airborne spread, Shiloh says. To look at this, he and his colleagues are now testing how easily M. tuberculosis strains with and without sulfolipid-1 are transmitted from infected guinea pigs to healthy ones. Understanding these pathways could pave the way to the development of targeted cough medicines that could help to prevent the spread of TB, he says.
Coughing is a symptom of many other contagious bacterial and viral infections, and how they may directly or indirectly stimulate cough probably varies to some extent, Shiloh says. Other members of the Mycobacterium genus, which can cause chronic cough in people with conditions such as HIV or cystic fibrosis, don’t make sulfolipid-1, so Shiloh is interested in finding out if these bacteria make their own, unique cough-triggering molecules. Research on Bordetella pertussis, which causes whooping cough, has begun to reveal a complex mechanism involving several molecules that work cooperatively to cause cough, but pathways for many other bacterial pathogens remain unclear.
Compared with bacteria, viruses have a very pared down genome, so they’re less likely to have the capacity to make specific molecules to cause cough and probably use other strategies, Shiloh says. Several respiratory viruses have been shown in animals and cell culture experiments to increase the production of receptors that trigger the cough reflex and boost infected animals’ sensitivity to cough stimuli.
Not all the signals to cough come directly from invaders. The body’s immune cells respond to respiratory infections – whether viral, bacterial or fungal – by secreting inflammatory molecules such as cytokines, prostaglandins and leukotrienes. These can cause cough by tweaking the receptors on airway sensory neurons, says Shiloh, who with Mazzone and coauthor Kubra Naqvi summarised the current understanding of how respiratory infections cause cough in the 2023 Annual Review of Physiology.
Why does a cough sometimes stick around for so long?
Even after viral infections are cleared from the airways, a cough can sometimes linger for weeks or even months, long after other symptoms have resolved. That’s likely in part because of residual low-grade inflammation in the respiratory system, Mazzone says.
But there’s also growing evidence from animal studies that viral infections, particularly when they’re more severe, can cause inflammation not just in the lungs but also in the long vagus nerve that runs between vital organs and the brain, carrying bundles of nerve fibres that regulate many basic functions, including the cough reflex. “That is thought to be a contributing factor to why some people have this persistent neuro-hypersensitivity that lasts much longer than the viral infection itself. It’s because those nerves remain inflamed, and that takes time to clear,” Mazzone says.
And that can keep a cough hanging around, often with heightened sensitivity, so that a smaller than normal stimulus – a whiff of perfume, a tiny amount of dust or smoke, even talking or laughing – triggers a cough.
What happens if the cough reflex doesn’t function properly?
Just as an overactive cough reflex can be problematic, so can an underactive one. The reflex is immature in young children – and that, combined with their propensity to put small objects in their mouths, puts them at greater risk of choking and aspirating things into their lungs, says pediatric pulmonologist Chang.
Foreign bodies can sometimes sit undetected in kids’ lungs for years, causing obstruction, inflammation and, incidentally, a chronic cough. Chang has removed nuts, beads and bits of sticky tape from children’s airways, and one time extracted a seashell that had been stuck in a teenager’s lungs for 14 years, causing a mysterious cough and airway damage. This is one reason it’s important not to ignore chronic cough, particularly in children, she says.
At the other end of the lifespan, the cough reflex can weaken in older adults, especially those with neurologic conditions like Parkinson’s disease. “They tend to have both a blunted sensation of the need to cough, and then also sort of discoordinated and weak cough air flows,” says Hegland, the speech-language pathologist. The dysfunctional cough reflex can contribute to the development of aspiration pneumonia, which is the leading cause of death in people with Parkinson’s.
So far, therapy for a weakened coughing function has focused on strengthening the muscles that contract to build air pressure and produce the forceful expiration of a cough, and this training has been shown to be helpful to an extent. But Hegland and collaborator Michelle Troche at Columbia University have also developed and tested a therapy that targets patients’ sensing of and response to a cough stimulus, with the goal of improving the cough reflex.
In a recent randomised controlled trial, Parkinson’s patients used either expiratory muscle training or the new sensorimotor therapy. Sensorimotor participants breathed through a face mask, through which they were given small amounts of aerosolized capsaicin, the same chemical that makes hot peppers spicy. Capsaicin also stimulates cough sensory neurons, and at the low doses used in the trial, causes a tickle at the back of the throat.
Upon feeling that tickle, participants were asked to produce a cough strong enough to reach a target airflow shown on a computer screen. The therapy allowed patients to practice noticing and responding appropriately to the sensory signals pinging from neurons in the respiratory tract.
In a 2022 study published in the journal Movement Disorders, Hegland, Troche and colleagues reported that both types of training improved Parkinson’s patients’ coughing abilities, but the sensorimotor training resulted in a greater urge to cough in response to the capsaicin stimulus and a stronger cough reflex. Hegland hopes that the therapy can help Parkinson’s patients keep their airways safe and find the Goldilocks of cough function: not too much, not too little – just right.
Courtesy: Science the Wire