Goa is abuzz with excitement as vintage bike and car owners, users, collectors and fans are decking […]
Old is Gold
October 4, 2016
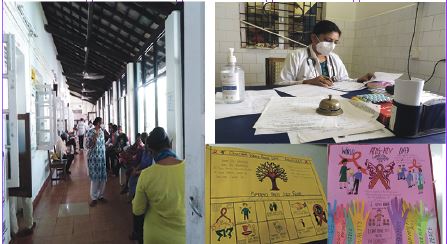
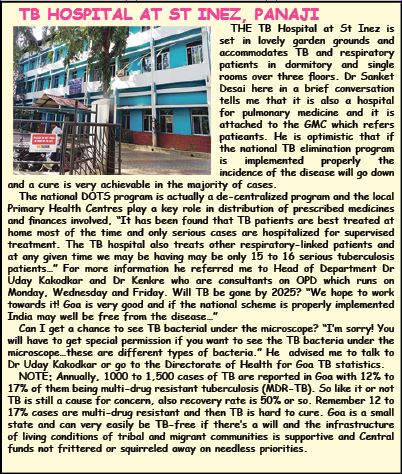
GLIMPSES OF THE CHEST DISEASES & TB HOSPITAL IN ST INEZ, PANAJI…where TB patients get timely advice and treatment. That’s Dr Lalitha Fernandes wearing a mask, she comes with ingenious ideas to make it easier for patients to take their TB medicines, posters up in her OPD clinic at the hospital, OPD happens on Mondays, Wednesdays and Fridays to screen patients with respiratory problems and TB. Goa sees about 1,000 to 1,500 patients of TB annually and the Central DOT regiment of treatment is run efficiently. Maybe by 2025 Goa will be TB-free!
By Pankajbala R Patel
WILL India be able to eradicate tuberculosis (TB) by 2025? Hardly likely! It’s a matter of shame that India still has the highest share of TB or tuberculosis infection in the world. Globally, this share is something like one-quarter! The top three countries still fighting TB in its populations are India (28%), Indonesia (9.2%, China (7,4%) and after that follow Philippines (7.06%), Pakistan (5.8%), Nigeria (4.4%), Bangladesh (3.6%), Democratic Republic of Congo (2.9%). In 2021 the estimated TB incidence was 2,59,000 – that is 188 per 1,00,000 population in India and that is indeed, a shocking figure. Out of this HIV positive TB incidence is as much as 53,000.
According to the Dr Lalitha Fernandes (pulmonary and respiratory medicine doctor of many years) at the Chest Disease & TB Hospital (part of the Goa Medical College & Hospital) at St Inez (Taleigao road) most of the TB patients they’re dealing with are HIV positive TB patients and many are drug-resistant, so it becomes that much uphill to treat them to achieve a cure…in 2021 an estimated 11,000 HIV positive patients died because of TB infection in India. The Global TB report has in 2021 altogether 4, 93,000 HIV patients dying worldwide. The TB burden continues to be huge so it is anyone’s guess if India which leads in TB incidence will be able to say goodbye to TB by 2025, although that’s what Union Minister of Health & Family Welfare JP Nadda wished for some time ago.
TB BACTERIAL INFECTION
WHILE TB is a bacterial infection which may infect any part of the body including the joint bones and even the skeleton, it is TB of the lungs or pulmonary TB which is most commonly contacted and feared. Pulmonary or lung TB is infectious and families with a TB patient at home have to take strict precautions isolating the patient until he/she is eventually cured – keeping feeding vessels and clothes for a separate wash, needless to say TB patients sleep in isolation so that their coughing does not spread to someone nearby. If it is a non-immune compromised TB patient who takes his TB medicines faithfully a cure is obtained in four to six months!
The fact is most patients find TB medicines very revolting – the all-in-one large magenta pink tablets are not very easy to swallow and patients who cannot swallow easily usually crush these tablets in water and swallow the pink slurry. But talking to Dr Lalitha Fernandes one discovered that they have ingeniously introduced a method of giving the medicine in an imaginative “sandwich fashion” – here patients eat whatever they want to eat with their tablets tucked into the food! This way they hardly realize they’re eating their medicines and eating them becomes more palatable, also side-effects of nausea and vomiting are less. It is a kind of applied psychology thinking which works once patients get used to the idea of tucking their tablets into a variety of food.
The very diligent Dr Lalitha, who says she been looking into TB treatments for over 35 years now, patients may even tuck the TB tablets (in broken pieces if need be) in a rava dosa or wrapped in a roti or in a sandwich with a filling — medicine is taken with every meal instead of independently one hour before a meal or after a meal. She says like this patients also improve their nutritional intake better, for better nutrition helps the patient recover faster. In the case of tuberculosis good nutrition is of the essence.
POOR NUTRITION
IT is not unknown that TB proliferates in closed, small, foetid homes where eating habits are poor and lacking in nutrient values. A large chunk of India’s urban population live in quarters damp and over-packed with extended family members – with very little quality of life. Although for that matter even in bigger richer households eating habits may be terrible and cold, damp homes are homes where infection sets in and spreads easily, especially if a family member contacts TB bacteria.
NATIONAL TB REGIMEN
WHAT is the national TB drug regimen like? TB is discovered in the exposure phase, latent phase and active disease phase and this is diagnosed with TB skin test and/or blood test which usually reveals the status of the much stigmatised disease. Reportedly, TB bacteria or mycobacteria grow slowly and die equally slowly too! The mycrobacteria divide asymmetrically, generating a population of cells that grow at different rate and of different size…depending on the severity of disease. Treatment is defined for the first phase of two months which is the intensive phase, then gradually tapered off over four to six months depending on the cure achieved and patients are no longer infectious.
TB DRUGS
WHAT are the drugs of TB? The most common active phase treatment is isoniazid INH in combination with three other drugs – rifapentine, pyrazinamide and ethambutol. One may actually feel better after the first two months although treatment usually continuous for six or more months. The finale phase of TB sees chest pain, persistent cough, loss of appetite, with sweat night sweats, fatigue and fever, a chronic hacking cough coming up with yellow, greenish mucus and the patient loses weight, suffers laboured breathing. Pulmonary TB patients suffer from persistent coughing which is worse at night.
Good nutrition can always make a difference to the recovery of a TB patient and usually patients are advised to eat fruit, porridge, peanut chikki, wheat and ragi preparations. In fact, the Central-government controlled DOT anti-TB drug regimen program is generous enough to offer TB patients under treatment Rs500 per month to eat a more nutritious diet, and another Rs500 goes to the caregiver who encourages the patient to stick to his TB medicines faithfully! However, who supervises whether the money is spent on buying milk, fruit and food or something else more desirable?
Will India be free of TB by 2025? It doesn’t look like and most of the medical staff engaged with the tuberculosis fight say we still have a long way to go before the living standards of below poverty level Indians improves enough to ensure that every Indian can afford the best of health food (which is also organically cultivated)! While the health of the educated and enlightened top brass of industry and society improves, not so rich Indians are still fighting for basic infrastructure to be healthy and happy.
And this is reflected in our TB statistics as well as the monsoon time demon diseases of malaria, dengue fever, chikengunya, thypoid fever and chronic amoebic dysentery. May the government see the light and sanction more funds for primary healthcare in its next national budget! India sees a barely two or marginally more financial budget for healthcare and in comparison with other countries is low down on the list.
 LETTER TO THE EDITOR FOR ISSUE DATED APRIL 11, 2026
LETTER TO THE EDITOR FOR ISSUE DATED APRIL 11, 2026 DOUBLE ENGINE GOA GOVERNMENT DANCES TO ADANI TUNES!
DOUBLE ENGINE GOA GOVERNMENT DANCES TO ADANI TUNES! WHO IS FIXING THE SKY? The billionaires, the cops in SUVs, and the missing trees! By Raaisa Lemos Vaz
WHO IS FIXING THE SKY? The billionaires, the cops in SUVs, and the missing trees! By Raaisa Lemos Vaz UPHEAVAL OF THE SUSEGAAD!By Sumaiya Khan
UPHEAVAL OF THE SUSEGAAD!By Sumaiya Khan THE POWER AND THE POLITICS OF MINING IN GOA!By Arvind Pinto
THE POWER AND THE POLITICS OF MINING IN GOA!By Arvind Pinto DEVA VANI DHRUPAD: Alchemy of Sound, Silence and Sanctity!By Prema Viswanathan
DEVA VANI DHRUPAD: Alchemy of Sound, Silence and Sanctity!By Prema Viswanathan AT LEAST HOSPITALS CAN OFFER MILLET ROTI AND KICHADI!
AT LEAST HOSPITALS CAN OFFER MILLET ROTI AND KICHADI! WHEN DO WE NEED PALLIATIVE CARE?
WHEN DO WE NEED PALLIATIVE CARE? GODI MEDIA TRUMPS TRUTH IN WAR & PEACE!
GODI MEDIA TRUMPS TRUTH IN WAR & PEACE! World Health Day 2026: TOGETHER FOR HEALTH – STAND WITH SCIENCE! By Dr Amit Dias, MD
World Health Day 2026: TOGETHER FOR HEALTH – STAND WITH SCIENCE! By Dr Amit Dias, MD FCRA AMENDMENT WILL ENABLE GOVT TO TAKE OVER PROPERTIES!By Olav Albuquerque
FCRA AMENDMENT WILL ENABLE GOVT TO TAKE OVER PROPERTIES!By Olav Albuquerque WEEKEND UPDATESLETTERS TO THE EDITOR FOR ISSUE DATED APRIL 04, 2026
WEEKEND UPDATESLETTERS TO THE EDITOR FOR ISSUE DATED APRIL 04, 2026 REAL ESTATE BARONS OF GOA!
REAL ESTATE BARONS OF GOA! THE SLOW VANISHING OF GOA’S GOLDEN BEACHES! By Raaisa Lemos Vaz
THE SLOW VANISHING OF GOA’S GOLDEN BEACHES! By Raaisa Lemos Vaz
Goa is abuzz with excitement as vintage bike and car owners, users, collectors and fans are decking […]